![]()
Advise

Information sharing: Sharing personally relevant information with your patient Information giving/ sharing is divided into content (what advice should I give?) and process (how should I give it?).
Process
There is a difference between unsolicited health advice, which can be annoying and patronising, and giving information that is tailored and wanted.
Always ask before you give advice. These scenarios below illustrate some common mistakes.
Scenario 1:

You need to lose some weight.

If they had only asked… I have just lost 3 kg.
Scenario 2:
You need to eat 5 portions of fruit and vegetable each day.
I know this already – this isn’t very helpful.
Instead try using the "permission, ask, provide, ask" (PAPA) framework.
Using the PAPA framework |
||
|---|---|---|
Permission |
|
|
Ask |
|
|
Provide |
|
|
Ask |
|
|
Content
It is also important to practise finding the right words. The PDF below gives some information on what to cover:
This printable PDF sheet gives some information content that patients might find helpful.
Click on the headings below to see examples of explaining health information in a patient-centred way and also what you should cover.
 Dietary advice:
Dietary advice:
Permission:
Would you like some information on the current recommendations on how to improve your diet?

Yeah, I suppose, that might be helpful!
Ask:
What do you know already about heathy eating?
Well obviously fruit and veg is good for you and take outs are bad! But it’s not always that easy in my busy life!
Provide/ Content:
There is strong evidence that people don't stick to crash diets for long and that they end up feeling bad about themselves as their weight goes up and down.
The NHS recommends manageable changes that patients can stick to for life. These changes include:
- How and when you eat, such as having regular meals away from the TV, eating with the whole family, and avoiding snacking;
- What you eat, so that you eat all the food groups in the right proportions and avoid soft drinks;
- How much you eat, through portion control. Some people find it helpful to use their hand as a guide to portion sizes. A clenched fist being an appropriate portion of carbohydrate (rice, pasta, bread) to have with each meal. [Eatwell plate with portion control ].
Aim for modest weight loss of up to 10% (average is 3%) at a rate of 0.5kg to 1kg per week, and then maintenance as a goal. Even slowing the rate of weight gain could be a helpful goal for some patients.
Ask:
Do you have any questions? Would you like to talk about any of these aspects in more detail?
Actually, yeah I never know how much is a good portion, so if you can help me with that ...
 Exercise advice
Exercise advice
Permission:
Would you be interested in some ideas for getting exercise despite your your knee pain?
Yes please, whenever I've tried to exercise in the past it's always flared up my knees, so it'll be nice to know what I should do.
Ask:
What kinds exercise or activities are you able to do comfortably at the moment?
Just short walks and I like dancing which doesn’t seem to bother my knees.
I don’t like running as I'm worried my knees might get worse if I 'over do it'.
Provide/ Content:
The NHS recommends 150 minutes of moderate exercise or 75 minutes of vigorous exercise each week. This is equivalent to 30 minutes moderate exercise 5 days a week, or 15 minutes vigorous exercise 5 days a week, plus strengthening exercises.
Try to be specific about how often, when, where and for how long you intend to exercise. [Exercise prescribing pad ]
Low impact exercise is beneficial for patients with wear-and-tear arthritis of their knees and hips. This can be explained as any exercise where no noise is made from impact e.g. cycling, swimming, yoga, pilates, rowing etc.
Ask:
What type of exercise do you think you could manage?
Zumba classes – once a week and walk once a week.
 Complex cases
Complex cases
Permission:
From what you have described I think we need to consider whether you might have something called binge eating disorder. Would you like some more information on this?

Yes, I guess so.
Ask:
Have you heard of binge eating disorder?
Yes, isn’t that where people feel out of control of how much they eat?
Provide/ Content:
Binge Eating Disorder (BED) is a condition that can be caused by many things, including low self-esteem or low confidence. People who have this disorder frequently eat uncontrollably until they feel unwell and may have feelings of guilt and shame. Many people get better after seeing a specially trained counsellor. Here is a leaflet / website.
Consider BED where there are three or more of the following:
- Eating much faster than normal during a binge
- Eating until uncomfortably full
- Eating a large amount of food when not hungry
- Eating alone or secretly due to being embarrassed about the amount of food consumed
- Feelings of guilt, shame or disgust after binge eating
Treatment involves addressing the psychological issues (through self-help e.g. www.b-eat.org.uk , psychological therapies such as CBT, and/or starting an SSRI) as well as a standard weight-loss plan once they are in control of their eating habits. BED has a good rate of remission with 50% responding to CBT treatment .
Ask:
Do you have any questions? Would you like some time to think about this further? Would you consider seeing someone for a more detailed assessment?
I think I’m going to look at that website and think about some of the advice it gives first. If I need any extra help I’ll come back for a referral.
 Health benefits
Health benefits
Permission:
Would you be interested in learning more about the health benefits of losing weight?
Yes, that might get me a bit more motivated.
Ask:
Are there any particular aspects of your health that you are concerned about?
Well yes, my blood pressure and my heart problems run in my family.
Provide/ Content:
There is strong evidence that losing a small amount of weight, or increasing the amount of exercise that you do can help to protect you from dementia / heart disease / cancer / diabetes / stroke etc. Here is a leaflet / website .
Most patients lose weight to look and feel healthier, and may be unaware of the health risks of obesity, or the benefits of modest weight loss. If your patient is already motivated, it may not be necessary to educated them, but if you feel they would benefit from understanding the health risks and benefits , tailor the advice to the areas of health that they are concerned about, perhaps due to family members with diabetes, arthritis, heart disease, or cancer. Try to couch this as education rather than advice (‘people who lose weight can significantly reduce their risk of many types of cancer’, rather than ‘you must lose weight to reduce your risk of cancer’).
Joint osteoarthritis
There is a strong and weight-related link with patients of BMI 35 have 14 times the risk of patients with normal BMI. Losing weight and low impact exercise has been shown to be as effective as surgery in symptom control. Useful patient leaflet
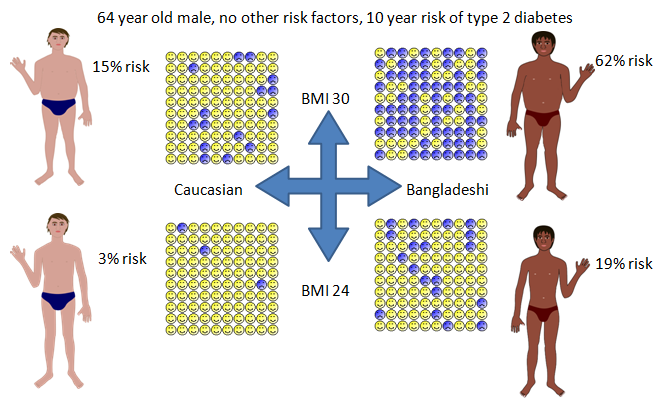
Type two diabetes
There is a strong weight-related link, with obese patients, and patients from some ethnicities (in particular the Indian subcontinent and some Afro-Caribbean populations) having dramatically higher levels of diabetes. Use this personalised risk calculator to illustrate your patient’s current level of risk and how losing weight could modify their risk.
Hypertension
Ask:
Would you like to discuss ways of achieving these health benefits?
That would be great!
 Advice for parents
Advice for parents
Permission:
Would you be interested in some of the recommendations for helping children be more healthy?

Yes, that would be helpful.
Ask:
Do you have any thoughts or concerns about helping your child be more healthy?
Well, I had a letter from school about Jonas’s weight. They said he was overweight, but I just put it down to the way he is built – he has always been on the chunky side.
Provide/ Content:
The NHS normally recommends that children don't try to lose weight, just to stop putting it on until they grown into a healthy weight for their height. Children can stop gaining weight by improving what they eat, eating child-sized meals, swapping snacks and sweet drinks for healthier options, and getting at least an hour running around every day. It helps if the whole family make changes together. Here is a helpful website.
Many parents are unaware that their children are overweight. It can help to be objective and to show where their child is on their height and growth chart (they should be in a similar centile for both). BMI tends to underestimate a child’s level of obesity, and a specialist paediatric healthy weight calculator should be used.
Young children should generally aim to ‘grow into their weight’ rather than lose weight. However as children approach their adult height, they will need to lose weight as an adult would.
Dietary change (e.g. cutting snacks and soft drinks) is the key intervention for severely overweight children as it has been shown that obesity causes inactivity rather than the other way around .
Ask:
What changes do you think you could realistically make? Would you like some more information on any of these aspects?
Well, he normally has a soft drink and a packet of crisps on his way home from school. I could try giving him water and a piece of fruit. He gets plenty of exercise I think. If I’m honest I probably give him adult-sized meals, and we always pressure him to finish his plate. I could try putting less on his plate and let him ask for seconds if he’s hungry.
 Causes of obesity
Causes of obesity
Permission:
Would you like some information on some of the causes of weight gain?
Isn’t it all down to our sedentary lifestyle?
Ask:
What do you feel is the main reason you put on weight?
Watching too much TV and driving to work.
Provide/ Content:
Weight gain is determined by a balance of energy in (food and drink) and energy out (exercise plus background metabolism). If people consume more than they expend, they put on weight. The reasons for excess calorie intake and inadequate calorie expenditure are complex and include differences in appetite, availability of food and snacks, unseen calories and some medical conditions.
The evidence shows that it is difficult to exercise enough to lose weight, unless you are controlling how much you eat at the same time. If exercise is difficult for someone, they can still lose weight by improving their diet, and reducing the amount that they eat.
Some medications can have a profound impact on appetite (e.g. valproate, lithium, olanzapine, risperidone, clozapine, amitriptyline, mirtazapine, cetirizine). Some medications cannot be withdrawn for clinical reasons, but others may be swapped for alternatives with less obesogenic effects.
According to the FOA the average UK calorie intake is 3,440 kcal while the recommended calorie intake is only 2,000kcal for women or 2,500 kcal for men. One hour’s vigorous exercise (more than most people do) consumes only about 500 kcal.
Ask:
What approaches do you think might work for you?
So exercise isn’t going to work off all those extra calories? I guess I need to start thinking about what I’m eating as well.
 Biomedical treatments - Orlistat
Biomedical treatments - Orlistat
Permission:
Would you like some information on Orlistat the weight-loss tablet?
Yes, please, that sounds really helpful.
Ask:
Have you heard of Orlistat before?
Yes, I think so. My friend tried it but stopped because it gave her side effects.
Provide/ Content:
Orlistat works by preventing the body from digesting fat. It therefore commonly causes faecal incontinence if fat is ingested. It is helpful if patients are able to stick to a fat-free diet, but many patients are intolerant of this side effect.
Some patients have the misconception that Orlistat will allow them to eat as much fat as they like without putting on weight. Orlistat effectively forces patients to adopt a fat-free diet.
Orlistat can be prescribed to patients with a BMI>30 (or 28 with risk factors), to be discontinued if the patient has not successfully lost 5% of their weight in 3 months.
Ask:
Is this something that you would like to try?
I don’t think I can realistically stick to a fat-free diet. And I don’t like the sound of diarrhoea. Perhaps I’ll try making changes another way.
Biomedical treatments - Surgery for weight loss
Permission:
Anita, as you meet our criteria for referral, would you like to know some more about weight-loss surgery?

Yes, please.
Ask:
What do you already know about weight loss surgery?
I know it is very effective. My neighbour had it done and lost lots of weight. Mind you, she says that she vomits if she eats more than a tiny amount.
Provide/ Content:
Surgery is the most effective treatment for obesity, however there are capacity issues (it is estimate that 5% of the UK population meets the current NHS criteria for surgery, but only 7,000 procedures are currently performed annually, creating a theoretical backlog of around 300 years). Newer therapies such as gastric balloons can be inserted gastroscopically as a day case but need to be removed 6-12 months later, but this service may not be available on the NHS in all areas.
Some patients have the misconception that surgery will allow them to eat as much as they like without putting on weight. Surgery effectively forces patients to eat smaller portions. Patients are referred to a tier 3 obesity service before being considered for surgery, where they receive coordinated exercise, dietary and psychological interventions.
Patients can be referred to this service if other treatments have failed if they have BMI >40 (or BMI>35 with comorbidities). It is used as a first line treatment if BMI >50.
Patients have to commit to life-long changes, and may develop nutritional deficiencies without life-long supplementation.
Ask:
Would you like to be referred to a specialist service for consideration for surgery?
I’m a bit frightened about surgery, but I’d be interested in knowing more about it. Can you give me a leaflet ?
Case Scenario: Advise Beverley

Patient Details
- Name: Beverley Buthelezi
- Age: 24
- Ethnicity: Black South African
- BMI: 35
- Family Background: family history of hypertension and heart disease
- Last Appointment: Recently attended for contraceptive advice, where you broached and booked a further appointment to talk about her health in general, having established her concerns about hypertension and heart disease.
1] Although Beverley is happy to discuss her weight, when asked if she has any concerns she states:
 “I’m not really bothered about my weight. My boyfriend likes me as I am. In my culture it is seen as unhealthy for a woman to be skinny.”
“I’m not really bothered about my weight. My boyfriend likes me as I am. In my culture it is seen as unhealthy for a woman to be skinny.”
What type of information would you like to share with Beverley?
Submit
You may want to share information about the health benefits of weight loss, in particular the effects on her cardiovascular health and blood pressure at this point.
Additional Activity
Practise finding the words using the PAPA framework.
2] Beverley also replies:
“I’d be happy, if losing a small amount of weight could mean that I didn’t need to start blood pressure tablets. However I don’t see how I can lose weight as I get sore knees every time I go for a run.”
What type of information would you like to share with Beverley?
Submit
You may want to share information on weight loss through dietary change and/or information on low impact exercise.
Additional Activity
Practise finding the words using the PAPA framework.